
Don’t Ignore Medicaid in Lobbying Efforts, Advocates Warned
 Advocates for public mental health services must pay more attention to Medicaid. That was the blunt message delivered at the June National Mental Health Association Conference (NMHA) by two experts on the subject.
Advocates for public mental health services must pay more attention to Medicaid. That was the blunt message delivered at the June National Mental Health Association Conference (NMHA) by two experts on the subject.
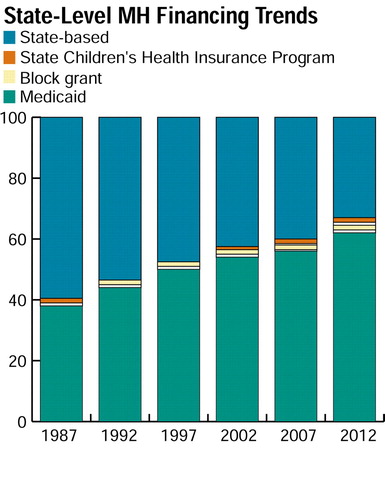
“Medicaid is becoming the primary source of funds for public mental health services,” said Jeffrey Buck, Ph.D., associate director for organization and financing at the federal Center for Mental Health Services (CMHS). “In 1987 funds from that program represented less than 40 percent of total public mental health funding. If current trends continue, that figure will climb to more than 60 percent by 2012.”
David Nelson, the NMHA’s vice president of health care reform, said, “Advocates have learned how to influence state mental health bureaucracies, but they have not always developed strong relationships with Medicaid agencies. A new advocacy role will become particularly important in times of budget deficits.”
John J. Wernert III, M.D., the Indiana Psychiatric Society’s (IPS) deputy representative to the APA Assembly, and other IPS members developed valuable experience with that new role when budget deficits threatened the pharmacy benefit to Medicaid recipients. As the governor’s appointee to the Indiana Medicaid Drug Utilization Review (DUR) Board (DUR), Wernert had an early warning about possible changes in the benefit.
“As is true in most states, the pharmaceutical costs to the Medicaid program have skyrocketed,” Wernert told Psychiatric News. “The DUR board was required by the governor’s office to cut over $80 million from the pharmacy benefit. Prior authorization became the method of choice to achieve those cost savings.”
Wernert and others were concerned that prior authorization strategies would be used on an “experimental” basis on psychotropic drugs. He believes that because of their high cost, psychotropic medications will always be a potential target of cost-cutting measures in state Medicaid programs.
As chair of the board of the Mental Health Association of Indiana, Wernert was in a good position to help build a broad coalition of organizations that have an interest in protecting access to psychotropic drugs. He and IPS legislative representative Stephen R. Dunlop, M.D., worked closely with Beth Karnes, president and chief financial officer of the Indiana Mental Health Memorial Foundation, to identify allies. In addition to the IPS, the coalition ultimately included consumer groups, family members, psychiatric nurses, psychologists, and other advocates.
Wernert said, “The professional and pharmaceutical industries will usually appear self-serving when they complain about prior authorization for restrictive practices relating to pharmaceuticals. Yet, when advocacy groups such as the Alliance for the Mentally Ill and the Mental Health Association use their grass-roots supporters, the legislators take notice.”
Coalition members also developed a broad approach to their advocacy. In a telephone interview, Karnes said, “Our strategy involved a four-pronged approach at the state level. Instead of merely focusing on key legislators and the governor, we targeted the state Medicaid and budget office as well. We made the argument to the Medicaid staff that the Olmstead decision [which requires that persons with mental illness be treated in the least-restrictive setting] would be difficult to implement without access to appropriate medication.”
He continued, “We encouraged the state budget office to look at the big picture.” Members of the coalition presented study findings showing that cost savings resulting from restriction of medication for persons with mental illness usually are more than offset by increases in spending by other service sectors.
The coalition achieved a partial victory when Senate Bill 471 passed both houses of the 2001 session of the Indiana General Assembly. That legislation stipulated that Medicaid recipients should be able to receive prescription drugs that are used for the treatment of a mental illness without any restrictions or limitations, including prior authorization, when the prescription drug is used for the treatment of a mental illness.
Governor Frank O’Bannon (D), however, vetoed the legislation, citing “cost considerations” and asked the Medicaid office to come up with other approaches to the problem. Coalition members plan to continue their struggles to ensure access to appropriate medication.
Wernert said, “There is no question in my mind that prior authorization as a cost-saving measure will be instituted in our Medicaid drug program. Our strategy is to make sure that psychotropics are the very last medications considered for prior authorization, not the first. Similar models in other states, like West Virginia, have well over 30 classes of medicines under prior authorization, but have not touched psychotropics.”
In a telephone interview, Buck expanded on his federal perspective about the increasing importance of Medicaid. “Mental health services are a relatively small part of the Medicaid program. Excluding funds spent on drugs, only about 10 percent of total Medicaid funds go to mental health.”
“So,” he added, “mental health is only one of many issues for Medicaid. But for anyone concerned about mental health, Medicaid is a 1,000-pound gorilla. We have to start thinking about how to integrate that program into the mental health system.”
At the state level, in Indiana, Wernert agreed. “It is already true that Medicaid is the primary source of funds for public mental health. [Its importance] will only continue in the future since most states have closed their state-sponsored institutions, and persons with chronic mental illness are living in the community and drawing Medicaid.”
He added a word of advice for other practitioners: “We must stay vigilant.”
Numerous reports on the topic of managed care and Medicaid are posted on the Web at www.mentalhealth.org/cmhs/managedcare/index.htm. Information on Indiana Senate Bill 471 can be accessed on the Web at www.ai.org/serv/lsa_billinfo by entering “471” in the “Go to Bill” box. ▪
