
Will-to-Live Profile Helps Tailor Cancer Patients’ Care
Living with death looking over my shoulder is a new experience,” a terminal cancer patient commented recently. But how does having “death looking over your shoulder” affect a terminal cancer patient’s will to live?
The answer is that it varies, with patients reacting in one of five different ways, a study reported in the October Psychosomatics suggests.
The study was conducted by Harvey Chochinov, M.D., Ph.D., a professor of psychiatry and family medicine at the University of Manitoba in Winnipeg, Canada, and Douglas Tataryn, Ph.D. As William Breitbart, M.D., chief of the psychiatry service at Memorial Sloan-Kettering Cancer Center in New York City, told Psychiatric News, the study is valuable because it deals with a subject that has not been addressed by psychiatric palliative care researchers, including himself.
Chochinov and Tataryn recruited subjects from patients newly admitted to the Riverview Palliative Care Unit in Winnipeg. All patients admitted to the unit at this time had a primary diagnosis of terminal cancer, notably terminal cancer of the lung or digestive systems. After admission, each patient was given 24 to 48 hours to adjust to the ward routine before being approached for the study. The patient’s medical status was then reviewed with the ward staff, and patients who were too cognitively impaired, weak, or ill to participate in the study were not approached. Also, not all of the patients asked to participate in the study wanted to participate. The researchers ultimately got 168 subjects, ranging in age from 31 to 89 years.
Twice daily until the end of their stay on the unit, the subjects took the Edmonton Symptom Assessment System, a self-report instrument consisting of a series of visual scales designed specifically for use with palliative patient populations. The average stay was 22 days. The scales assess pain, anxiety, depression, a sense of well-being, shortness of breath, nausea, activity, drowsiness, and appetite. For this study, an additional will-to-live visual scale was added.
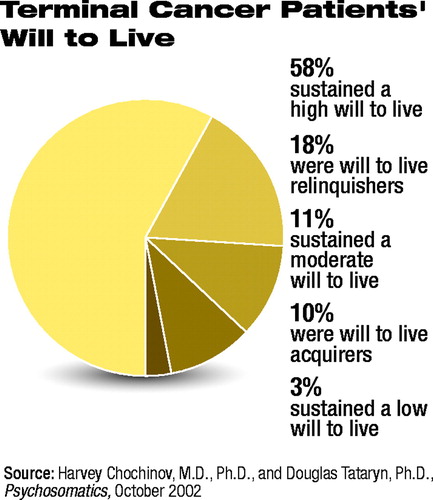 The investigators then statistically analyzed the data to ascertain the pattern of each subject’s will to live over time. They found that the subjects fit one of five different will-to-live trajectory profiles. Ninety-five (58 percent) of the subjects had sustained a high will to live; 29 (18 percent) were will-to-live relinquishers; 19 (11 percent) had a sustained moderate will to live; 16 (10 percent) were will-to-live acquirers; and five (3 percent) had a sustained low will to live.
The investigators then statistically analyzed the data to ascertain the pattern of each subject’s will to live over time. They found that the subjects fit one of five different will-to-live trajectory profiles. Ninety-five (58 percent) of the subjects had sustained a high will to live; 29 (18 percent) were will-to-live relinquishers; 19 (11 percent) had a sustained moderate will to live; 16 (10 percent) were will-to-live acquirers; and five (3 percent) had a sustained low will to live.
Chochinov and Tataryn also determined the extent to which membership in each of the five will-to-live profiles could be explained by initial symptom characteristics and patient demographic variables. For instance, subjects with sustained high will to live had the lowest levels of anxiety, were more likely to be religious, and had the lowest prevalence of colon cancer. Subjects who acquired will to live over their hospital course had the highest prevalence of colon cancer, were admitted with the highest levels of nausea, were most likely to be living with a partner, and were most likely not to be religious. Subjects with sustained low will to live had the highest levels of anxiety—more than three times that of the group with sustained high will to live; the highest levels of shortness of breath (about three times that of the other groups); and the lowest rate of living with a partner.
Some of these discoveries, Chochinov explained to Psychiatric News, should help both psychiatrists and family physicians “improve the quality of palliative care provided to patients approaching death.”
For instance, the fact that subjects with sustained high will to live had low levels of anxiety and tended to be religious suggests that finding ways to control anxiety and to provide spiritual support might be valuable components of high-quality end-of-life care for terminal cancer patients. Since the will-to-live acquirers had the highest prevalence of colon cancer and the highest level of nausea upon being admitted to the palliative unit, it suggests that even for those nearing death, pharmacological relief of nausea might very well help patients reestablish a will to live.
Other of their findings, Chochinov and Tataryn pointed out in their report, may be relevant to the controversy over physician-assisted suicide. For instance, previous studies suggested that patients who wanted to end their lives through physician-assisted suicide suffered considerably from anxiety and lack of social support, like the sustained low will-to-live subjects. Thus, one way to help such patients might be to alleviate their anxiety and bolster their social support, Chochinov and Tataryn believe.
Some of the study’s results also imply that the will to live might influence survival in terminal cancer patients. Specifically, those with a sustained moderate will to live lived longest, on average 190 days after being admitted to the unit, and those with a sustained low will to live died soonest, on average 28 days after being admitted to the unit. However, as Chochinov explained to Psychiatric News, these findings should be treated with extreme caution as he and Tataryn did not set out to study survival and as they did not control for variables that might have influenced survival.
The study was funded by the National Cancer Institute of Canada, the Canadian Cancer Society, and the Project on Death in America of the Open Society Institute.
The study, “Predicting the Trajectory of Will to Live in Terminally Ill Patients,” is posted on the Web at http://psy.psychiatryonline.org/cgi/content/full/43/5/370. ▪
Psychosomatics 2002 43 30
