
Plan to End Medicaid Payments Threatens Teaching Hospitals
APA is strongly protesting a proposed rule by the federal Centers for Medicare and Medicaid Services (CMS) that would eliminate Medicaid payments for graduate medical education at teaching hospitals.
A proposed rule published May 23 in the Federal Register would prohibit states from receiving federal funds under the Medicaid program in any manner that could be construed as payment related to a provider's graduate medical education (GME) costs.
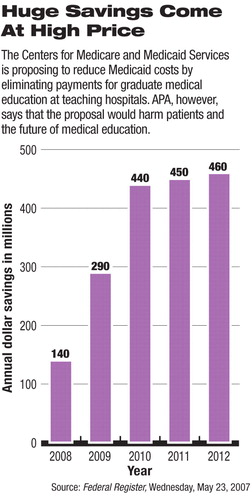
By CMS's estimates, implementation of the rule would save the federal government hundreds of millions of dollars over the next five years (see chart).
But in comments submitted to CMS, APA said that these savings would come out of the budgets of the nation's teaching hospitals, many of which treat the poorest patients while training future doctors.
APA also stated that CMS is trying to assert statutory authority in prohibiting states from seeking Medicaid GME payments, despite the fact that the government has been allowing such payments for years.
“The position articulated within this proposed rule represents an unsupported 360-degree turnaround in CMS's longstanding policy of approving payment under Medicaid to compensate providers for GME-related costs,” APA said. “While CMS poses a variety of rationales for this complete reversal to Medicaid GME payments, none are legally supported or persuasive. The clear intent of the proposed rule is simply to cut out providers' GME-related payments to gain substantial cost savings. CMS estimates the cuts at $290 million for the first full fiscal year, 2009, and much more thereafter.”
In a letter from APA Medical Director James H. Scully Jr., M.D., APA pointed out that “it is teaching hospitals that will lose this money that has been used to help offset the many expenses associated with teaching medical students.” Teaching hospitals commonly serve inner-city populations with large Medicaid and Medicare caseloads, as well as large proportions of nonpaying patients, he continued, and the substantial funding cut that would result from the proposed rule would adversely affect the financial welfare of any hospital that has been able to offset its teaching expenses with Medicaid GME payments.
“Since many inner-city hospitals have for years experienced considerable financial strains that have resulted in closures, an additional cut to their Medicaid payments is counter to public policy,” Scully told CMS.
GME Payments Hard to Track
In the proposed rule, CMS states that GME “is not a health service that is included in the authorized coverage package. Nor is GME recognized under the Medicaid statute as a component of the cost of Medicaid inpatient and outpatient hospital services.”
CMS referenced a 2003 state survey conducted by the Association of American Medical Colleges (AAMC) that found that 47 states and the District of Columbia reported using Medicaid funds to make GME payments. “Of these, 35 indicated that the payments were included in their perdiem inpatient hospital rates, and 15 started using supplemental or a combination of supplemental and per-diem payments to make GME payments,” CMS stated.
“This same report.. .indicates that while states view these Medicaid GME payments as critical to state GME policy implementation, they generally do not track these payments,” CMS said.
“In large part, this inability to track Medicaid GME payments is due to the way in which these payments are made,” CMS asserted.“ Basically, payments are made through increases in the rates paid for covered Medicaid services. This methodology assures federal participation, but does not provide clear accountability. Funding intended by the states to support GME often becomes subsumed within [managed care organization] or hospital rates (including supplements to these rates) or inpatient disproportionate share hospital (DSH) payments. As a result, it is difficult to quantify Medicaid GME payments or monitor and measure the effect of Medicaid payments on GME programs.”
If the proposed rule is implemented, CMS estimates that it would reduce federal Medicaid outlays by $140 million in Fiscal 2008, $290 million in Fiscal 2009, and as much as $460 million by Fiscal 2012.
APA Suggests Alternative
APA, however, urged CMS to consider alternatives, including promulgation of rules that would enhance the accountability of states to track and monitor GME-related expenses. “Many federal programs support states in their education and training of upcoming physicians because this is an essential activity needed to preserve national public health and welfare.”
The AAMC also has registered a protest against the proposed rule.
“Many major teaching hospitals share a special mission in treating large numbers of Medicaid and uninsured patients,” stated Robert Dickler, senior vice president of the AAMC's Division of Health Care Affairs, in a letter to CMS. “Representing only 6 percent of all hospitals, major teaching hospitals are the sites for approximately a quarter of all Medicaid discharges. Indeed, our nation's teaching hospitals provide large amounts of ambulatory care in poor communities, often acting as the 'family doctor' in areas where few individual practitioners exist, accept Medicaid as a form of payment, or provide charity care.
“Eliminating Medicaid GME payments would significantly threaten the ability of teaching hospitals to continue these activities,” Dickler stated. “The result would be to severely undermine the infrastructure of the American health care system.”
The proposed rule is posted at<http://a257.g.akamaitech.net/7/257/2422/01jan20071800/edocket.access.gpo.gov/2007/07-2576.htm>.▪
